The post Including Men in Breast Cancer Studies appeared first on Dr Deanna Attai.
]]>Last week, the US Food and Drug Administration (FDA) issued draft guidelines for industry, which encourage the inclusion of male breast cancer patients in clinical trials that evaluate breast cancer therapies. The guidelines note that “eligibility criteria for clinical trials of breast cancer drugs should allow for inclusion of both males and females” and that “scientific rationale should be included in the protocol when proposing to exclude males from breast cancer trials.” There is a 60-day open comment period on the guideline.
In the US, approximately 2600 men are diagnosed with breast cancer each year, approximately 1% of all new breast cancer cases. Men tend to be diagnosed at more advanced stages compared with women, and there are about 500 male breast cancer related deaths in the US annually. Breast cancer in men is usually treated in a similar manner as in women. However, because men are typically not included in breast cancer clinical trials, it is not known if this is an optimal approach. One of the primary reasons that men are excluded from breast cancer clinical trials is that the disease is uncommon – setting up a vicious cycle where little progress is made. The statement noted that “FDA does not intend to consider low expected accrual rates of male patients with breast cancer to be a sufficient scientific rationale for excluding them from a clinical trial.”
This is most certainly a welcome step towards improving the understanding and treatment of male breast cancer.
- Forbes: FDA Urges Inclusion of Men in Breast Cancer Clinical Trials
- CureToday: FDA Encourages Men to be Included in Breast Cancer Clinical Trials
The post Including Men in Breast Cancer Studies appeared first on Dr Deanna Attai.
]]>The post Screening Mammography in High-Risk Men appeared first on Dr Deanna Attai.
]]>There are no standard guidelines for mammographic screening for men who have no symptoms (such as a lump), even if they are considered to be at high risk for developing breast cancer. A study recently published in Breast Cancer Research and Treatment* evaluated the performance of screening mammography in asymptomatic high risk men.
The researchers reviewed a prospective institutional database at the Memorial Sloan Kettering Cancer Center, evaluating cases from 2011 – 2018. 827 men underwent mammography during that time period, but 80% were excluded from evaluation for this study as they underwent imaging due to the presence of a mass or other symptoms. Data from 163 asymptomatic patients, considered high risk due to a family and/ or personal history of breast cancer or the presence of a deleterious genetic mutation, was analyzed.
Of the 163 men, 77% had personal history of breast cancer and 44% had a family history of breast cancer. 15% had deleterious BRCA mutations. Most of the genetic mutations (83%) were in the BRCA2 gene, as expected.
Over the 7-year time period, 806 screening mammography examinations were performed. The majority (792 studies, 98%) were BIRADS 1 or 2, indicating a normal study or benign findings. 10 (1.2%) were BIRADS 3 indicating a “probably benign” finding. Upon follow up, all of these patients were considered to have benign findings. 4 men had BIRADS 4 or 5 findings indicating suspicious or highly suspicious findings for which biopsy was recommended, and all were diagnosed with invasive ductal breast cancer.
Breast cancers in men are often diagnosed at more advanced stages than in women, and as a result, outcomes may be poorer. The authors noted that while mammographic screening has not been shown to reduce breast cancer mortality rates (the reason screening is performed) in men, the detection rate in this high-risk population (4.96 per 1000 examinations) is comparable to the breast cancer detection rate from screening mammography in average risk women. There were no false-positive (“false alarm”) biopsies in this group. The authors acknowledged one of the primary limitations of their study, the relatively small number of patients, and called for larger studies to confirm their findings. They concluded that their study “suggests that screening mammography should be performed in men at increased risk for breast cancer.”
*If you are not able to access the full study and would like a copy, please email me: contact at drattai dot com
The post Screening Mammography in High-Risk Men appeared first on Dr Deanna Attai.
]]>The post Breast Conserving Therapy for Male Breast Cancer appeared first on Dr Deanna Attai.
]]>Note – if you would like a copy of the studies discussed below but are not able to access them from the journal website, please email me: contact at drattai dot com
In a study recently published in the Annals of Surgical Oncology, Bateni et al used the National Cancer Database to assess outcomes in patients with male breast cancer based on surgical therapy. The authors found improved 10-year survival in patients who underwent breast conserving therapy (BCT) which they defined as partial mastectomy (also called lumpectomy) plus radiation therapy.
Male breast cancer makes up about 1% of all new breast cancer diagnoses; approximately 2500 men are diagnosed in the US each year. Treatment guidelines for male breast cancer are similar to those for post-menopausal women despite growing evidence that breast cancer in men is a biologically different disease versus that in women. One of the challenges for clinical trials is the relatively small numbers of male breast cancer patients diagnosed each year. However, many clinical trials have not included men.
A total of 8445 patients with stage I and II breast cancer, treated between 2004-2014, were included for analysis. 61% underwent mastectomy, and 18% underwent BCT. 12% had mastectomy with radiation, and 8% had partial mastectomy without radiation. Median follow up was 52 months. At 10 years, overall survival was as follows:
- 74% BCT
- 58% mastectomy
- 56% mastectomy with radiation
- 56% partial mastectomy without radiation
The image below is Figure IA from the manuscript, which show the “crude” overall survival for male breast cancer patients depending on surgical therapy.
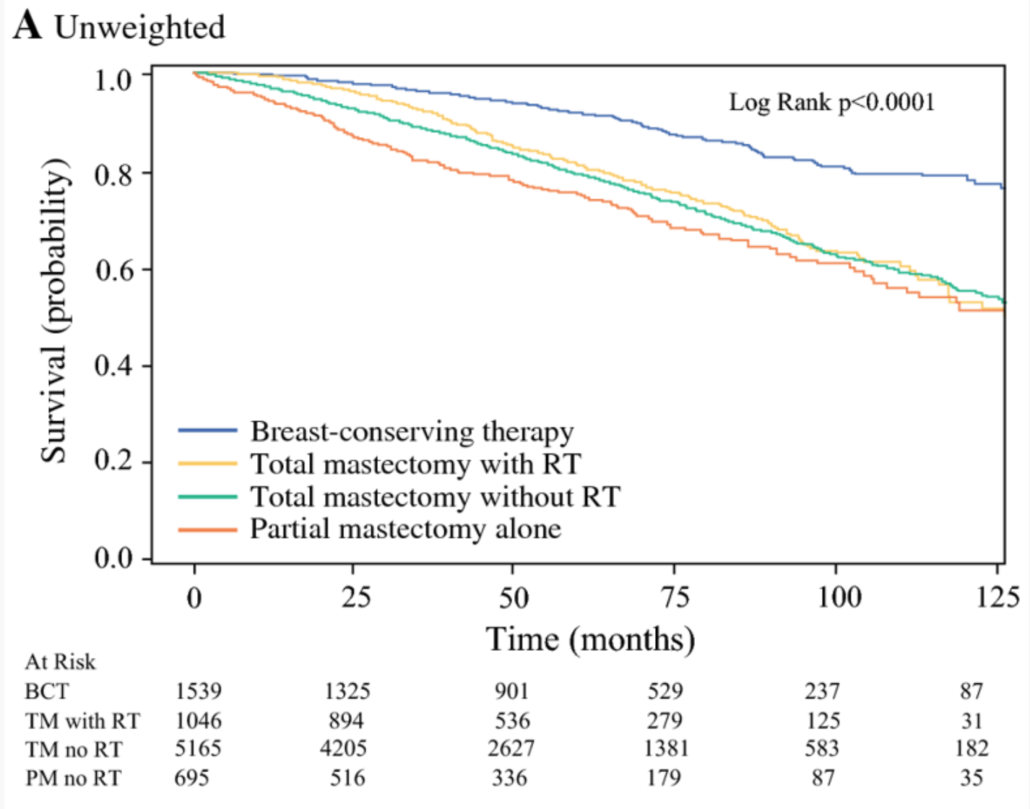
Evaluating patients who had breast conservation with or without radiation, the authors noted that patients who were older, had higher tumor stage, higher cellular grade, and triple negative histology had poorer overall survival rates. They noted that there were differences in patient age, co-morbidities (other medical conditions), margin status and chemotherapy use for patients who underwent BCT versus partial mastectomy alone. However, after accounting for these differences, survival rates still favored BCT, suggesting that radiation therapy is an important component of improved outcomes.
Limitations of the study noted by the authors include the retrospective nature, and the inability to understand some of the factors that influenced the decision for mastectomy versus breast conservation. Her2/neu status was not uniformly reported in the NCDB until 2010, so almost half of the patients in this study did not have this information. They also noted a larger percentage (4.9 vs 1.4%) of patients in the BCT group had triple negative breast cancer, which might explain why more of these patients were also treated with chemotherapy. It is also not clear how much of an influence the use of chemotherapy and endocrine therapy had in terms of the survival rates that were noted.
In a separate article, De La Cruz et al performed a systematic literature review of the studies evaluating breast conservation in men (excluding the Bateni et al study discussed above). The authors found 8 publications meeting their criteria. Among these studies, there were 859 patients who underwent breast conservation, 14.7% of all male breast cancer surgeries in the combined papers. Reporting on the “weighted average”, local recurrence (cancer returning in the breast) was 9.9%, disease-free survival was 85.6% and 5 year survival was 84.4%. As with the retrospective database analysis, there are limitations to this type of literature review – studies may use the same data points for inclusion, including use of radiation therapy, chemotherapy, and margin status. There may be significant differences in the patient populations in the various studies reviewed. As in the Bateni et al paper, there may be multiple unknown factors that influenced a decision for surgery type.
Men tend to present with larger tumors, especially relative to breast size, so often mastectomy is recommended. However, the authors of both papers were of the opinion that breast conservation is oncologically safe and a very reasonable option for men with early stage breast cancer, if they desire. Bateni et al stressed the importance of radiation therapy if breast conservation is utilized. Both papers highlight the importance of clinical trials for male breast cancer, so that treatment recommendations can be based on the best available evidence.
Additional information on Male Breast Cancer:
The post Breast Conserving Therapy for Male Breast Cancer appeared first on Dr Deanna Attai.
]]>The post Endocrine Therapy for Breast Cancer – Research Survey appeared first on Dr Deanna Attai.
]]>Note – the survey closed on July 7th 2019. Thank you to all who participated and shared, and we will be sure to post the results when they are available!
Approximately 25-30% of patients with breast cancer who are prescribed endocrine therapy do not complete the full course of treatment, and some patients never start. Side effects of endocrine therapy are well documented but there is very little literature on the role of the medical team in helping patients manage treatment-related side effects.
This survey is being conducted for research purposes. It is a UCLA research survey, open to women and men with a history of breast cancer who have been treated with or who have received a recommendation for endocrine therapy.
This survey is voluntary and is completely anonymous – no identifying information, including internet protocol (IP) addresses, will be collected. The survey should take approximately 15 minutes to complete. We value your time and your opinions.
For questions regarding this study, you may contact principal investigator Dr. Deanna Attai By phone: (818) 333-2555; by email: [email protected]; or by mail: 191 S. Buena Vista #415, Burbank, CA 91505
UCLA Office of the Human Research Protection Program (OHRPP):
If you have questions about your rights as a research subject, or if you have concerns or suggestions and you want to talk to someone other than the researchers, you may contact the UCLA OHRPP By phone: (310) 206-2040; by email: [email protected]; or by mail: Box 951406, Los Angeles, CA 90095-1406
The post Endocrine Therapy for Breast Cancer – Research Survey appeared first on Dr Deanna Attai.
]]>The post Updates from #SSO2019 appeared first on Dr Deanna Attai.
]]>The Society of Surgical Oncology held their annual meeting in San Diego, CA from March 27-30, 2019. Approximately 1700 surgical oncologists were in attendance. As the organization is geared towards the entire field of surgical oncology, only a portion of the meeting covered breast cancer. Here are some of the highlights:
Genetic Testing and Management
Dr. Judy Garber – Dana Farber
Updates in Testing and Management of BRCA Mutations
– BRCA Mutation information from the National Cancer Institute
– Consider repeat testing if original genetic testing was performed prior to 2012 as more genes as well as pathogenic mutations have been discovered
– NCCN guidelines for breast cancer surveillance in BRCA 1/2 mutation carriers:
o Clinical breast exam every 6-12 months starting at age 25
o Annual MRI age 25-75 (individualize after age 75)
o Annual mammogram age 30-75 (individualize after age 75)
– NCCN guidelines for breast cancer prevention in BRCA 1/2 mutation carriers: discuss mastectomy, discuss tamoxifen
– Premenopausal BRCA mutation carriers who undergo oophorectomy experience breast cancer risk reduction. The level of breast cancer risk reduction in BRCA1 carriers is lower than in BRCA2 carriers as BRCA1-associated tumors are more likely to be triple negative
– Prenatal genetic testing is available in mutation carriers, and may be used for selective reproduction
– BRCA 1/2 mutation status does not impact breast cancer outcomes; tumor biology impact on outcomes is independent of mutation status
– BRCA 1/2 are DNA repair genes. Tumors associated with BRCA 1 tend to be triple negative and tumors associated with BRCA 2 tend to be ER/PR+, Her2- (but all combinations have been seen)
– Clinical trials are evaluating the use of cisplatin chemotherapy in patients with BRCA mutations – cancer cells are not able to repair DNA-induced chemotherapy damage due to the defective BRCA gene
– PARP inhibitors interfere with DNA repair and have traditionally been used to treat ovarian cancer. Small studies show some effect in breast cancer in the setting of BRCA mutations. Larger studies are ongoing. So far they only seem to work in breast cancer when there are BRCA mutations
– A challenge to treatment with PARP inhibitors is that there are many mechanisms of resistance, and tumors demonstrate a variable response to therapy – tests are being developed to predict response
– Lurbinectedin – a drug from sea slugs (!) may have some effect
– A very interesting comment – Dr. Garber noted that DNA breaks may be immunogenic, so there may be a role to combine PARP inhibitors and immunotherapy treatments
– Denosumab, a RANK-ligand used for bone protection in breast cancer patients, may have breast cancer risk-reducing activity – a randomized trial is pending to assess its activity as a preventative agent
Thuy Vu, Genetic Counselor – Wake Forest
What Genetic Test Should I Order?
– Once the appropriate patient for genetic testing has been identified, how to decide what lab to use? Consider lab experience, as well as cost and insurance support
– Patients with a complicated family history (multiple different cancers in scattered relatives), absent family history (adopted), and evidence of multiple cancer syndromes will benefit from NGS (next-generation sequencing) genetic panel testing
– A disadvantage of broad genetic panel testing is that there is currently incomplete information on all of the mutations that may be identified. Risk for cancers unrelated to the current diagnosis may be identified. In addition, there will be an increased prevalence of variants of uncertain significance (VUS)
– She noted to use caution when patients bring in test results from ancestry.com and similar companies – these sites often assess for SNPs (single nucleotide polymorphisms), which is not the same as testing for a genetic mutation, and full genetic testing may need to be repeated
– She acknowledged that there is a shortage of genetic counselors, even in large university centers. Many testing companies and labs now have associated genetic counselors, and there are some independent companies offering telephone counseling services
Dr. David Euhus – Johns Hopkins
ATM, CHEK2 and Other Genes
– While multiple gene mutations influencing breast cancer risk have been identified, they do not all convey the same level of risk
– As testing for multiple genes has increased, BRCA mutations are no longer the most common mutations found
– High risk genes include BRCA 1/2, TP53, PTEN, PALB2, STK11, CDH1
– Moderate risk genes include ATM, CHEK2, NBN, NF1
– These and other genes explain approximately 14-28% of genetic risk for breast cancer – most patients with a strong family history of breast cancer do not have an identifiable mutation
– There is a range of risk associated with all of the genes that in part depends on the mutation type – what type of damage does the mutation cause to the DNA. Family history of breast cancer can modify risk.
– For most of these patients, NCCN guidelines recommend annual MRI in addition to mammograms. Age to start supplemental screening depends on the mutation.
– He noted that increased screening for other associated cancers when there is no clinical benefit leads to patient harms – financial, emotional, and physical
– A good question from the floor about the role of ultrasound as supplemental screening (in addition to MRI) – Dr. Euhus states he uses 3D mammogram / tomosynthesis and does not use ultrasound unless the patient is pregnant / lactating
Dr. Kevin Hughes – Massachusetts General Hospital
What the Surgeon Needs to Know about Genetic Testing
– High cost of testing is not the problem – interpretation of the results is the challenge
– Assuming that approximately 10% of breast cancers are hereditary, over 51,000 breast cancers could have been prevented with testing
– For the breast surgeon, understanding BRCA 1/2 is not enough. There are many genes, each have different spectrum of associated cancers and associated risk; treatment needs to be individualized for the patient taking into account their specific mutation and family history
– He emphasized the point Dr. Garber made that if testing on a breast cancer survivor was performed prior to 2012, those patients should be re-tested
– Recent American Society of Breast Surgeons guidelines call for consideration of genetic testing in all breast cancer patients
– Dr. Hughes notes that this is already a standard recommendation for other cancers such as ovarian, pancreas and others
– The field is becoming more complicated – it is not expected that anyone can memorize this – go to the internet and look it up!
Resources:
ASK2ME – All Syndromes Known to Man Evaluator
ClinVar – look up specific mutations to see how they have been classified
PROMPT registry for patients with rare mutations
Breast Cancer Treatments in the Young and Elderly
Dr. Mina Sedrak – City of Hope
Treatment Strategies in Octogenarians with Early Stage, High-Risk Breast Cancer
– Incidence and mortality from breast cancer increase with age; the number of older adults in the US is increasing
– Breast cancer outcomes are often worse for older (as well as younger) women
– Older adults are underrepresented in cancer clinical trials – 1/3 of patients with breast cancer are over the age of 70, but only a small percentage of them are included in clinical trials
– Because of lack of clinical trial data in older women, patients may be under- or over-treated [DJA note – we have a similar situation in men with breast cancer].
– There is no universal definition of “old”. Aging is a continuous spectrum, and chronological age does not accurately predict functional age. The ASCO Guidelines Geriatric Assessment can help understand factors other than chronological age to predict morbidity and mortality. US Life Tables can also be used to estimate life expectancy, as well as ePrognosis. Estimation of life expectancy should be performed for all older patients before making a treatment plan
– How to best treat cancer in the elderly patient: it depends on life expectancy, aging concerns, risks / benefits of treatment and the potential impact of co-existing medical problems
– What risks can we modify and what are the patient preferences? There is no “one size fits all”
Dr. Tyler Chesney – University of Toronto
Adjuvant Radiotherapy for Older Women after Breast Conserving Surgery
– 4 randomized clinical trials addressed if elderly patients with low-risk breast cancer need radiation therapy after breast conserving therapy: NSABP B-21, A. Fyles, CALGB 9343, and PRIME II studies
o Meta-analysis of these 4 studies: 2387 patients across all trials, early stage breast cancer, hormone receptor positive. Addition of radiation therapy reduces local recurrence from 60 versus 10 / 1000 at 5 years. 2 trials had 10 year follow up, noting recurrence was 80 versus 20 / 1000 women.
o 3 of the trials provided data on axillary recurrence: absolute benefit was small, 12 versus 3 / 1000 women. No difference in distant recurrence or overall survival
– Prime I study showed that older women who underwent radiation therapy had increased fatigue over 5-10 years but similar overall health-related quality of life
– Accelerated partial breast irradiation may be an option, but some studies have shown higher local recurrence and poorer cosmetic result (depending on treatment method)
– While toxicities of radiation therapy have improved with more modern techniques, logistical concerns such as time, need to travel, and cost may be of higher concern for older women
Dr. Laura Dominici – Dana Farber Cancer Institute
Reconstruction and Body Image in Young Patients
– More than 13,000 women under the age of 40 are diagnosed with breast cancer annually in the US, approximately 7% of all new diagnoses
– Younger women newly diagnosed with breast cancer have been shown to have higher rates of anxiety and distress after diagnosis, they have historically received more aggressive treatment, and have a long survivorship period
– More aggressive surgery such as mastectomy does not lead to improved overall or breast cancer specific survival. Local recurrence is related to tumor biology, not age of the patient
– Mastectomy (single and bilateral) rates are rising, especially among younger women. Rates of reconstruction are increasing, as are rates of post mastectomy radiation
– A growing number of patients are “going flat” after mastectomy, opting for no reconstruction
– Dana Farber young women’s multicenter prospective cohort study: poorer satisfaction with breast-related, psychosocial and sexual well-being after unilateral and bilateral mastectomy. Other factors impacting poorer satisfaction include financial status, lymphedema, and the need for radiation
– 42% of women age 50 and younger (in the Dana Farber study) regret their surgical decision including primary surgery and reconstruction decision. Patients in this study were not asked what the actual regret was – doing too much or too little
– Important for patients to understand the oncologic outcomes of their decisions, and for physicians to promote shared decision making that takes into account patient preferences and concerns
Dr. Jo Chien – University of California, San Francisco
Fertility in Young Breast Cancer Patients
– 51% of women under age 40 with breast cancer are concerned about fertility; 38% desire to have future children but up to 97% are at risk of treatment related infertility. 26% report that their concerns about infertility affected their treatment decisions
– Loss of reproductive potential after cancer treatment results in worse long-term quality of life, unresolved grief / depression, reduced life satisfaction. Fertility preservation associated with less regret among young cancer survivors
– Less than 25% of general oncologists refer young breast cancer patients to fertility specialists
– Factors impacting risk of chemotherapy-induced ovarian failure: older age, baseline ovarian reserve, type of chemotherapy, and chemotherapy dose / duration
– Menses is not a surrogate marker for fertility. Fertility decline occurs ~10 years before onset of menopause. For women who remain premenopausal after chemotherapy, the majority enter menopause prematurely
– Options for fertility preservation: ovarian stimulation and cryopreservation of embryos / oocytes, GnRH agonists, and experimental techniques such as cryopreservation of ovarian tissue and immature oocyte retrieval with in vitro maturation
– Several studies have evaluated safety of letrozole-gonadotropin protocol in women with breast cancer and have found no difference in relapse-free survival. Very limited data on safety of ovarian stimulation in the neoadjuvant setting. In subset (82 patients – 34 stimulation / 48 controls) of I-SPY2 trial, no delay in start of neoadjuvant treatment and no significant difference in pCR or recurrence or mortality rates in patients who underwent ovarian stimulation before chemotherapy
– As discussed in the genetics session, Dr. Chien noted that for BRCA mutation carriers, pre-implantation genetic diagnosis is an option. Multiple follicles / embryos are required, often needing multiple stimulation cycles
– Observational studies suggest that pregnancy is safe after breast cancer.
– When is it safe to become pregnant after treatment? It comes down to patient’s underlying risk and likely their risk aversion. Dr. Chien prefers to wait to 2-3 years, but notes there is no data to support that. The POSITIVE trial is studying the impact of adjuvant endocrine therapy interruption to allow for pregnancy
Key papers
Dr. Kandace McGuire from Virginia Commonwealth University Massey Cancer Center provided an overview of 3 practice-changing papers from 2018. She noted at the start of her talk that while this is a surgical audience, all of the studies were from the medial oncology literature. This comment highlighted the multidisciplinary nature of breast cancer care – the entire treatment team needs to be aware of the latest advances and updates.
The TAILORx study assessed Oncotype Dx results and noted that many patients previously classified as intermediate risk could now be classified as low risk. Therefore, a larger percentage of patients do not need chemotherapy. However, questions remain for patients under the age of 50.
The TEXT / SOFT trials evaluated the use of ovarian suppression in premenopausal women with hormone receptor positive breast cancer. Ovarian suppression resulted in improved disease free and overall survival, but the magnitude of improvement varied according to recurrence risk. High risk patients may have 10-15% improvement. However, quality of life and fertility may be impacted by ovarian suppression in these younger women
The KATHERINE study assessed the use of TDM1 in patients with Her2/neu over-expressed tumors who did not exhibit a pathologic complete response (pCR) after neoadjuvant (before surgery) chemotherapy. Those who received adjuvant TDM1 versus trastuzumab showed an improved disease free survival, but more study is needed to assess the effect on overall survival.
Dr. V. Craig Jordan delivered the American Cancer Society / SSO Basic Science Lecture: The SERM Saga: Something From Nothing. Dr. Jordan’s presentation was a nice history lesson about the discovery and use of tamoxifen as a treatment for breast cancer.
– Dr. Jordan noted the early clues that endocrine therapy might be effective for some breast cancers – removal of the ovaries, adrenal glands, and even part of the pituitary gland led to improved outcomes (with a fair amount of associated risk)
– Tamoxifen was initially developed as a contraceptive agent, but it was not successful and was going to be discarded by the manufacturer
– The link to endometrial cancer and tamoxifen was initially denied, despite some interesting studies by Dr. Jordon noting the association. He noted that the early studies evaluating tamoxifen simply did not assess for endometrial cancer
– He noted that the cumulative frequency of uterine cancer with 2 years of tamoxifen is ~1.5%, and with 5 years of tamoxifen ~5.5%. He commented that if the studies were performed today, the data monitoring committees would “go apoplectic” over these results
– Raloxifene in early studies showed decrease in breast cancer but also decrease in bone fractures – this led to the STAR trial which assessed the ability of raloxifene and tamoxifen to reduce breast cancer development in high-risk women
– He discussed other drugs, derived from tamoxifen, that are being developed – searching for those with improved side effect profiles
– He quoted George S. Patton: “If everyone is thinking alike, then someone isn’t thinking”
Presidential Address – Serendipity and Strategy on the Path of Progress
Dr. Armando Giuliano, known to some as the “father” of the sentinel node biopsy, provided some interesting details on how his research process unfolded. He noted that “my success has been due to good luck, mixed with hard work, strategic planning, and serendipity.” Like those before him who proposed less aggressive surgical therapy for breast cancer, he was met with a fair amount of criticism. Patients and surgeons have benefited from his perseverance and dedication.
All of the research abstracts and posters can be found here. There were many interesting and thought-providing presentations, but it is important to remember that abstracts have not been subject to the peer-review process, and may represent incomplete data.
As usual if anyone is interested in one of the articles but does not have access, please send your email address to me: contact at drattai dot com and I will be happy to send you a copy.
This post has not been endorsed by the Society of Surgical Oncology.
The post Updates from #SSO2019 appeared first on Dr Deanna Attai.
]]>The post New Patient Information Website appeared first on Dr Deanna Attai.
]]>9 November 2015
The American Society of Breast Surgeons Foundation has just launched a patient information website – Breast360.org. The site was developed by breast surgeons, and patient advocates have had input and oversight during the entire process. Please take a look, and feel free to provide feedback if you have a suggestion for additional content.
The post New Patient Information Website appeared first on Dr Deanna Attai.
]]>The post Prophylactic Mastectomy for Male Breast Cancer appeared first on Dr Deanna Attai.
]]>I asked Dr. Oliver Bogler, a male breast cancer patient and advocate, to provide his perspective as a male breast cancer patient and cancer researcher.
Guest post by Dr. Oliver Bogler
The observation published in JAMA Surgery (doi:10.1001/jamasurg.2015.
By way of a brief background, men make up about 1% of breast cancer patients, and given the relative lack of knowledge about the male form of the disease, they are clinically managed like women with overall good outcomes. Men are typically diagnosed later (older and with more advanced stage) probably because awareness lags behind women and there is of course no screening, but grade for grade we do as well as women. Men can also be predisposed to having breast cancer by BRCA mutations, and are more commonly associated with BRCA2. I’ve written more on the biology of biology of tumor suppressor genes and familial predisposition on my blog and so won’t go into any detail here. Suffice it to say, that as far as we know today, which admittedly isn’t far enough, male breast cancer looks a lot like female breast cancer.
I think it is therefore reasonable to consider whether the reasons why men chose prophylactic contralateral mastectomies are the same that motivate women to make this choice. The report by Jemal and colleagues doesn’t look at BRCA status (data not available) nor does it examine the attitudes that having breast cancer and/or a BRCA mutation inform in people so affected. Excellent work in this latter area is being done by, for example, Dr. Sharlene Hesse-Biber, who has written on women in this context (Waiting for Cancer to Come) and is actively researching men. (Disclosure: I have participated in Dr. Hesse-Biber’s research work as a subject.)
Until we know the full answer of what drives men’s decisions on mastectomy, we can perhaps consider anecdotal evidence: I spoke with a man just last week who made exactly this choice after he learned from the analysis following his first mastectomy, that he was a BRCA2 mutation carrier. His rationale: same as women. He felt that his remaining breast was not useful and it had an elevated risk of growing a tumor, so why not remove it. Why wait for the tumor to grow first?
I think it is therefore most likely that the increase in genetic testing, particularly for BRCA, is driving the increase in men’s prophylactic contralateral mastectomies. For women access to affordable, effective reconstruction is probably a contributing plus, but for men this is not likely, as we rarely opt for this choice.
Are the number out of proportion? In the Huffington Post Dr. Jemal is quoted as saying ‘”[The operation] is only
Perhaps Dr. Jemal is arguing that it only makes sense to remove the contralateral breast when the stage of breast cancer is considered curable by surgery alone i.e. at stage I or less. Men admittedly are more often diagnosed at stage II, or even III and IV, and by definition we are talking about men with a diagnosis of cancer and already one mastectomy under (over?) their belt i.e. not people who have a predisposition but no cancer diagnosis, like Ms. Jolie. I understand this biologically: if you are stage II and above the cancer cells are on the move to a greater or lesser extent, and the focus must be on regional control with radiation and systemic control with chemo and hormone therapy, as appropriate. These approaches are aimed at keeping the cells hiding throughout your body at bay. But if we knew where a bunch of likely cells were hiding with a high likelihood, and it was in a very accessible place and in tissue that wasn’t useful, wouldn’t we simply remove them surgically?
Of course the key to this question is data in the form of large cohort studies – ultimately we will want to know whether men with BRCA mutations did better if they had the prophylactic contralateral mastectomies than if they didn’t, both in terms of overall survival and disease free survival. My guess is that it will be a long time before such a study can be done, even retrospectively, in men, so we will look to the women for guidance. Of course over there they haven’t quite agreed on the value of a mammogram yet, so we won’t hold our breath. In the meantime, if it was me (and it isn’t – I do not have BRCA mutations) I would gladly turn the other breast.
 Dr. Oliver Bogler is a former cancer researcher and male breast cancer patient and advocate. He writes about his experience and issues related to male breast cancer at Entering a World of Pink.
Dr. Oliver Bogler is a former cancer researcher and male breast cancer patient and advocate. He writes about his experience and issues related to male breast cancer at Entering a World of Pink.
The post Prophylactic Mastectomy for Male Breast Cancer appeared first on Dr Deanna Attai.
]]>The post Male Breast Cancer: Facts and a Personal Perspective appeared first on Dr Deanna Attai.
]]>Guest Post by Dr. Oliver Bogler
When thinking about a post on male breast cancer, one person came to mind – Dr. Oliver Bogler. As a cancer researcher, Dr. Bogler has a very unique perspective on his diagnosis, treatment, and the larger problem of research disparities when it comes to male breast cancer. Here is his guest post:
My personal encounter with breast cancer started with my diagnosis in September of 2012. My story is very typical. As I have written more extensively about it elsewhere let me be brief: I felt a lump, and after a few months of denial I had it checked out, and then very quickly was diagnosed and treated at MD Anderson Cancer Center in Houston, where I also work. More on that below, but let’s first look at some facts about the male disease.
About Male Breast Cancer
Approximately one in every hundred people diagnosed with breast cancer is a man. That’s about 2,200 new cases a year in the USA. Men have breasts, meaning that they have the same lobular glands and ducts that women have, though they have less tissue and it does not produce milk. Accordingly, male breast cancer is typically ductal carcinoma and hormone receptor positive and Her2 negative, which is also the most common type of breast cancer in women. Men are diagnosed later in life, typically, with a median age at diagnosis of 68, or about 7years older than women. For that reason men also present more often with more advanced forms of breast cancer – stages III and IV are more common, and stage I very rare. One possible explanation is that a lack of awareness results in delayed diagnosis, and so more advanced presentation at a later age.
Treatment regimens for men are essentially identical to those used for women, and outcomes are very similar, as far as we know. Because male breast cancers are typically hormone receptor positive, hormone therapy with the anti-estrogen tamoxifen is commonly an important part of the therapy. It suppresses male estrogen, and thereby other hormones also, which are co-regulated, including testosterone.
Many websites, including those of the American Cancer Society and the National Cancer Institute provide fundamental information about male breast cancer. Interventional clinical trials on breast cancer that men are eligible for can be found here (ClinicalTrials.gov is a registry and results database of publicly and privately supported clinical studies of human participants conducted around the world).
My advice: if you feel a lump, any lump, go see a doctor right away.
My Journey – Our Journey
One of the reasons I hesitated to get my lump checked out was that my wife had been diagnosed and treated for breast cancer about 5 years before me. I couldn’t really grasp the improbability of it hitting our nuclear family twice. Being Irene’s care taker and then a patient allows me to say with confidence that the treatments for men and women are identical: we both had up-front chemotherapy in a two step regimen: 12 rounds of weekly Taxol and then 4 rounds of the combination FAC at three week intervals. MD Anderson physicians prefer to give the chemo first as it provides an opportunity to see how the tumor responds. Then we both had surgery – modified radical mastectomy with axillary lymph node dissection – followed by 6 weeks of radiation to the chest wall. Now we both take hormone therapy – aromatase inhibitors for Irene, good old tamoxifen for me. Evidently we feel that marriage is all about sharing experiences 
What we know about male breast cancer and opportunities to learn more
What do we know? Probably not enough. I do accept that the treatment men receive is effective – there are some relatively small-scale, hospital registry based studies showing this. When adjusted for age and stage at diagnosis, it looks like men do as well as women with today’s approaches. On the other hand, the possibility that a sex-hormone driven cancer may have important differences between men and women cannot be excluded. Very encouraging is a current, larger registry trial in a network of European and US cancer centers with about 1,200 men that will provide a robust baseline outcomes data set and afford the opportunity to collect tissue and study the disease. It is the kind of research that was being done 20+ years ago in women.
An analysis I wrote about on my blog and in Breast Diseases Quarterly [Bogler, O. (2013) Male Breast Cancer: Opportunities for Research and Clinical Trials. Breast Diseases: A Year Book Quarterly 24(3), 216-218] suggests that there is very little primary research on the male disease. There are no laboratory models, cell lines or other tools. Few if any grants supporting this kind of fundamental biology are in evidence, and aside from the inclusion of male breast cancer in the epidemiology of rare cancers it is hard to find any support for research from the National Cancer Institute or foundations. Given that the NCI alone spends $600M on breast cancer research, there is in my mind ample opportunity to dedicate some to this question. Perhaps 1% would be a good start?
On a similar note, men are only eligible for about 30% of breast cancer clinical trials found on clinicaltrials.gov, suggesting that access is a real issue. Of course in some instances our inclusion may not make sense, but I believe that in many instances inertia rather than a biological rationale underlies the exclusion of men. Both of these areas provide significant opportunities to learn more about the male disease and how best to deal with it clinically.
The Awareness Gap
Being a man with what is widely understood to be a women’s cancer leads to some dissonant experiences. To me these are mostly mildly funny, and not an issue – being asked how I get a mammogram for instance (the same way you do…), or filling out a form that asks me whether I am pregnant or when my last period was. Its fine – I get it. Mostly women here, and mostly the men in the waiting room aren’t wearing the medical arm band. But having breast cancer as a man is still (local) news worthy, and has modest shock value – that is surprising. The issue here is that a lack of awareness is probably a contributing factor to the delayed diagnosis in men and that means in some cases in their earlier death. It is certainly contributing to the underfunding of research and exclusion of men from trials. We need to change that.
A key challenge for men with breast cancer is the phenomenal success of the breast cancer awareness community. While the excesses of “pink” are unfortunately common these days, I do acknowledge the amazing work the community has done, and am deeply grateful for it. Alone the fact that we can have frank, open discourse about breast cancer, any cancer, is a tribute to the brave women who came out with their disease in the past 50 years. Then, the mobilization of public and private resources for awareness, screening and research is a tremendous accomplishment. And the US is a clear leader in this – a significant cultural accomplishment. But if this huge silver lining has a tiny, tiny black cloud it is that pink leaves almost no room for awareness about men. Breast cancer actually is not a sex-specific cancer like ovarian, uterine, testicular or prostate – it just appears to be. A great illustration of this phenomenon for me is the NFL players who in October don pink in support of women with breast cancer (hurray!) and completely fail to take the opportunity to also mention that they themselves could be diagnosed with this disease one day (booo!).
I want to close by being clear: I am not advocating for male breast cancer at the expense of other forms of breast cancer. Not at all. I want it to have its place with, and alongside. And in proportion – 1% would be a good start. Perhaps my concerns are not dissimilar from those of the inflammatory, triple negative or metastatic breast cancer communities: being outside the pink mainstream presents awareness challenges, which in turn make it harder to gain the resources needed to change the fate of many women and men with breast cancer.
Dr. Oliver Bogler is a cancer researcher, male breast cancer patient, and male breast cancer advocate. His blog can be found at Entering a World of Pink.
The post Male Breast Cancer: Facts and a Personal Perspective appeared first on Dr Deanna Attai.
]]>The post Breast Cancer Diagnosis and Treatment, BRCA Testing, PinkWashing, and More! appeared first on Dr Deanna Attai.
]]>This is one of my most comprehensive interviews to date. It aired on Santa Clarita Valley TV and I had the opportunity to discuss a wide range of topics, including breast self-exams, male breast cancer, genetic testing for breast cancer, “pink washing” and more! Many thanks to SCVTV as well as Tami Edwards and Dave Caldwell, for spending so much time on such important topics.
The post Breast Cancer Diagnosis and Treatment, BRCA Testing, PinkWashing, and More! appeared first on Dr Deanna Attai.
]]>